The 2024 McDonald criteria represent the most significant shift in MS diagnosis in decades, introducing advanced MRI biomarkers like the Central Vein Sign (CVS) to reduce misdiagnosis and enable earlier detection. These breakthrough imaging techniques, proven through the landmark CAVS-MS trial where QMENTA's platform enabled multi-site standardization, promise to transform how clinical trials approach MS patient identification and enrollment. Here's what research leaders need to know about implementing these game-changing diagnostic tools in their imaging workflows.
The diagnostic journey for multiple sclerosis (MS) has reached a pivotal moment. For decades, the McDonald criteria have been the cornerstone of MS diagnosis, evolving to expedite the diagnosis of MS and thereby improving clinical outcomes. A persistent challenge has been the rate of misdiagnosis, often due to the non-specific nature of white matter lesions seen on conventional MRI. Advances in understanding of MS over the years have now led to a substantial revision of the McDonald criteria (1,2), providing a consolidated approach to expedite the diagnosis of MS, aiming for worldwide applicability while preserving specificity.
The main changes introduced in the new 2024 McDonald criteria(1) are the following:
- Unified approach: for diagnosing multiple sclerosis in individuals with relapsing or progressive courses throughout the lifespan.
- Diagnosing Before Clinical Symptoms: A major shift allows for a formal MS diagnosis in certain individuals with Radiologically Isolated Syndrome (RIS) who show characteristic MRI or other biomarker evidence. Rooting the diagnostic criteria in the biological mechanisms of MS.
- Prioritizing Dissemination in Space over Time: The criteria now include the optic nerve as a fifth location to help prove dissemination in space (DIS), and the requirement for dissemination in time (DIT) is now considered non-essential.
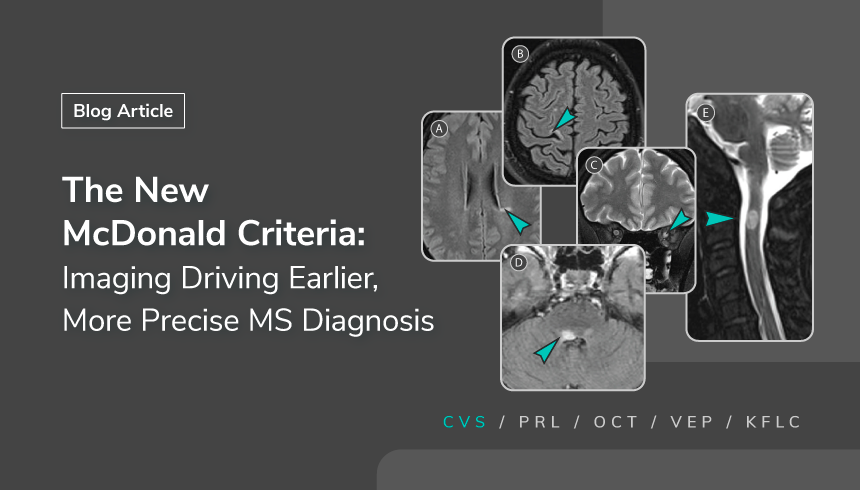
- Improved Accuracy with MRI: Advanced MRI biomarkers, such as the Central Vein Sign (CVS) and Paramagnetic Rim Lesions (PRLs) can be used to diagnose MS in specific situations.
- Expanded Biomarker Options: The use of kappa free light chains (kFLC) in the CSF is now interchangeable with oligoclonal bands (OCBs) in the context of clinical and MRI findings. kFLC is more accessible, quantitative, and faster.
Signal vs. Noise: Imaging Biomarkers in the New McDonald Criteria
Previous iterations of the McDonald criteria excelled at improving diagnostic sensitivity, allowing for earlier detection based on the pattern of lesion dissemination in space (DIS) and time (DIT) (3). However, the white matter hyperintensities detected by conventional MRI sequences are not pathognomonic for MS. This diagnostic "noise" is the primary driver of misdiagnosis. The 2024 revisions introduce two powerful biomarkers that isolate the "signal" of true MS pathology, each visualizing a distinct and fundamental aspect of the disease process.
Central Vein Sign (CVS): A Window into MS Pathology
The histopathological hallmark of MS is perivenular inflammation. The disease process begins when inflammatory infiltrates, rich in T- and B-lymphocytes, form "cuffs" around small post-capillary venules within the central nervous system's white matter. This targeted, perivenular attack is the initiating event of demyelination and lesion formation.
The central vein sign is the direct in vivo visualization of this foundational pathological event. Using susceptibility-sensitive MRI sequences, such as T2∗-T2-weighted imaging or a composite sequence known as FLAIR∗, neuroradiologists can identify the small central vein as a hypointense (dark) line or dot within a hyperintense (bright) MS lesion. See the detailed description of the
CVS workflow in our previous article.
This direct link between pathology and imaging is what gives the CVS its exceptional diagnostic power. While other conditions can cause white matter lesions, they do not typically originate from this specific perivenular inflammatory process. Clinical validation studies have established robust quantitative thresholds for its use. In fact, with a cutoff of 40–46% of an MS individual's white matter lesions being CVS-positive, the CVS reaches a sensitivity of 95% and a specificity of 92% for differentiating MS from its mimics (4, 5). The high specificity of the CVS as a non-invasive marker for MS gives clinicians an unprecedented level of diagnostic confidence.
Paramagnetic Rim Lesions (PRL): An Emerging Biomarker
Alongside CVS, the new McDonald criteria also recognize paramagnetic rim lesions (PRLs). These lesions reflect chronic, smoldering inflammation and have shown strong specificity for MS in research settings. While PRLs are not yet widely operationalized in clinical workflows, their inclusion signals the growing role of advanced MRI biomarkers in diagnosis.
QMENTA’s Role: Scaling Imaging Biomarkers for Clinical and Research Use
The McDonald Criteria have flagged CVS as a biomarker to boost diagnostic confidence. To achieve this, its utility had to be proven in a real-world, multi-site setting, which was the central goal of the
CAVS-MS trial (9). Within this landmark collaboration, involving leading researchers like with Dr Daniel Ontaneda (Cleveland Clinic) and Dr Pascal Sati (Cedars-Sinai), neuroradiologists faced significant hurdles: a lack of standardized techniques and the difficulty of simultaneously evaluating both MS lesions and the tiny veins within them.
QMENTA’s Imaging Hub was designed to solve these exact problems. Our platform provided the critical infrastructure that not only centralized all trial data but also delivered an AI-powered, semi-automated workflow that standardizes the entire process, including:
- Automated Image Processing & Standardization: The platform automatically validates incoming data, converts images (DICOM to NIfTI), aligns them to a standard space, and generates specialized FLAIR* images—eliminating the site-to-site variability that typically plagues multi-center trials. A neuroradiologist performs a final quality check to ensure consistency.
- AI-Powered Lesion Segmentation: An AI algorithm automatically identifies and maps white matter lesions, reducing the time radiologists spend on manual segmentation while maintaining accuracy. This map is then reviewed and refined by a human image analyst, combining efficiency with expert oversight.
- Centralized Data Management & Quality Control: A unified data repository with built-in quality metrics, automated data validation rules, and comprehensive audit trails addressing the chaos of managing imaging data across multiple sites while ensuring regulatory compliance and data integrity for trial submissions.
- Interactive CVS Detection Workflow: A radiologist uses an intuitive marker tool to identify central veins within lesions. The interface creates a clickable list of all marked veins and their coordinates for easy navigation and review, streamlining what was previously a time-intensive manual process.
- Standardized Data Capture & Export: All findings, including lesion counts, volume, and separate assessments for dissemination in space/time (DIS/DIT), are automatically captured in standardized formats and exported as trial-ready metadata, eliminating the manual data compilation that typically delays study timelines.

Figure1: QMENTA´s CAVS-MS Workflow
At QMENTA, we are incredibly proud to have played a key role in the inclusion of the Central Vein Sign (CVS) in the 2024 McDonald criteria. This milestone was made possible through the landmark CAVS-MS trial (9), and our cloud platform was the engine that enabled multiple institutions to collaborate seamlessly and to prove the undeniable value of CVS to the world. Now that the criteria are established, our mission is to empower the next wave of discovery, helping sponsors of clinical trials and leaders of clinical research centers. The path forward involves:
- Contact and Consultation: Engage with a specialized imaging platform provider like QMENTA for a demonstration and to discuss the specific needs of your trial or clinical program.
- Pilot Program: Initiate a pilot study to validate the advanced imaging protocols on your institution's scanners and to familiarize your research team with the analysis workflow in a low-risk environment.
- Starter Kit and Integration: For organizations with internal data science capabilities, leverage a Software
- Development Kit (SDK) to integrate proprietary algorithms or customize workflows within a validated, compliant platform ecosystem.
The new 2024 McDonald criteria herald a new era in MS diagnosis, one defined by biological precision and technological enablement. By embracing these advancements, the clinical and research communities can work together to reduce misdiagnosis and improve outcomes for people living with MS.